Pulmonary Embolism: What Patients and Clinicians Should Know
Introduction
Pulmonary embolism is a potentially life‑threatening condition and a priority for emergency and preventive healthcare. Understanding its causes, symptoms and pathways to diagnosis matters for clinicians, hospital administrators and members of the public alike. Timely recognition and treatment can markedly reduce complications and mortality, while effective prevention reduces hospital stay and long‑term disability.
Main body
What it is and why it occurs
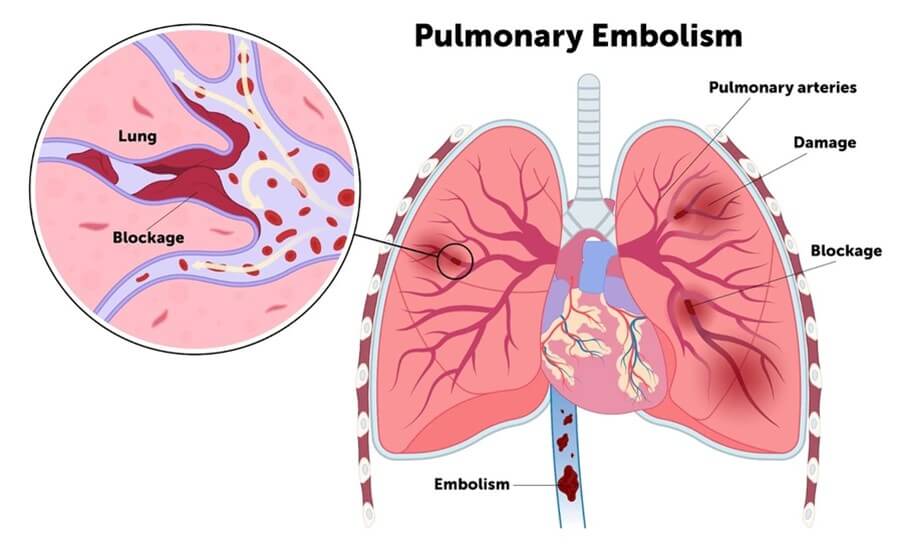
A pulmonary embolism occurs when material — most commonly a blood clot from the deep veins of the legs — travels to and blocks an artery in the lungs. This can impair oxygen delivery and place strain on the right side of the heart. Clots frequently originate from deep‑vein thrombosis (DVT) and share many of the same risk factors.
Common signs and risk factors
Symptoms often include sudden breathlessness, chest pain that may worsen on breathing, a cough (sometimes with haemoptysis), faintness or rapid heart rate. Risk factors include recent surgery or trauma, prolonged immobility (for example after long travel or during hospital admission), active cancer, pregnancy and the postpartum period, use of oestrogen‑containing medications, obesity and inherited clotting disorders. Age and smoking also increase risk.
Diagnosis and acute management
Diagnostic evaluation typically includes clinical assessment supported by tests such as D‑dimer blood assays and imaging — most commonly CT pulmonary angiography or ventilation–perfusion scanning where appropriate. Compression ultrasonography may identify the source DVT. Initial treatment focuses on anticoagulation to prevent clot growth, using heparin and oral anticoagulants. In cases of large or life‑threatening emboli, thrombolysis or surgical intervention may be considered.
Prevention
Prevention strategies in hospitals and community settings include early mobilisation, mechanical measures such as graduated compression stockings or intermittent pneumatic compression, and pharmacological prophylaxis for people at elevated risk.
Conclusion
Pulmonary embolism remains a serious but often preventable cause of acute deterioration. For readers, the key messages are awareness of symptoms, seeking urgent care for sudden breathlessness or chest pain, and adherence to prevention measures during periods of immobility. For health services, ongoing emphasis on risk assessment and rapid diagnostic pathways will continue to improve outcomes.